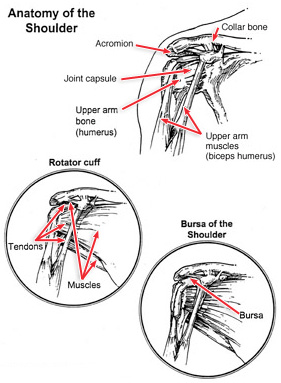
Common Shoulder Injuries
Warning Signs of a Shoulder Injury
Common Shoulder Injuries
Rotator Cuff Injuries
Treatment of Shoulder Injuries
Shoulder injuries are frequently caused by athletic activities that involve excessive, repetitive, overhead motion, such as swimming, tennis, pitching, and weightlifting. Injuries can also occur during everyday activities such washing walls, hanging curtains, and gardening.
Warning Signs of a Shoulder Injury
If you are experiencing pain in your shoulder, ask yourself these questions:
• Is your shoulder stiff? Can you rotate your arm in all the normal positions?
• Does it feel like your shoulder could pop out or slide out of the socket?
• Do you lack the strength in your shoulder to carry out your daily activities?
If you answered "yes" to any one of these questions, you should consult an orthopaedic surgeon for help in determining the severity of the problem.
|
|
| |
|
Common Shoulder Injuries
Most problems in the shoulder involve the muscles, ligaments, and tendons, rather than the bones. Athletes are especially susceptible to shoulder problems. In athletes, shoulder problems can develop slowly through repetitive, intensive training routines.
Some people will have a tendency to ignore the pain and "play through" a shoulder injury, which only aggravates the condition, and may possibly cause more problems. People also may underestimate the extent of their injury because steady pain, weakness in the arm, or limitation of joint motion will become almost second nature to them.
Orthopaedic surgeons group shoulder problems into the following categories.
Instability
Sometimes, one of the shoulder joints moves or is forced out of its normal position. This condition is called instability, and can result in a dislocation of one of the joints in the shoulder. Individuals suffering from an instability problem will experience pain when raising their arm. They also may feel as if their shoulder is slipping out of place.
Impingement
Impingement is caused by excessive rubbing of the shoulder muscles against the top part of the shoulder blade, called the acromion.
Impingement problems can occur during activities that require excessive overhead arm motion. Medical care should be sought immediately for inflammation in the shoulder because it could eventually lead to a more serious injury.
Rotator Cuff Injuries
The rotator cuff is one of the most important components of the shoulder. It is comprised of a group of muscles and tendons that hold the bones of the shoulder joint together. The rotator cuff muscles provide individuals with the ability to lift their arm and reach overhead. When the rotator cuff is injured, people sometimes do not recover the full shoulder function needed to properly participate in an athletic activity.
Treatment of Shoulder Injuries
Early detection is the key to preventing serious shoulder injuries.
Shoulder Exercises
Often, an orthopaedic surgeon will prescribe a series of exercises aimed at strengthening the shoulder muscles.
Here are some easy shoulder exercises that you can do to strengthen your shoulder muscles and prevent injuries.
Basic shoulder strengthening
Attach elastic tubing to a doorknob at home. Gently pull the elastic tubing toward your body. Hold for a count of five. Repeat five times with each arm. Perform twice a day.
Wall push-ups
Stand facing a wall with your hands on the wall and your feet shoulder-width apart. Slowly perform a push-up. Repeat five times. Hold for a count of five. Perform twice a day.
Shoulder press-ups
Sit upright in a chair with armrest, with your feet touching the floor. Use your arms to slowly rise off the chair. Hold for a count of five. Repeat five times. Perform twice a day.
Other Treatment
Anti-inflammatory medication also may be prescribed to reduce pain and swelling.
Shoulder Joint Tear (Glenoid Labrum Tear)
Anatomy
Risk Factors/Prevention
Symptoms
Diagnosis
Treatment
Rehabilitation
Advances in medical technology are enabling doctors to identify and treat injuries that went unnoticed 20 years ago. For example, physicians can now use miniaturized television cameras to see inside a joint. With this tool, they have been able to identify and treat a shoulder injury called a glenoid labrum tear.
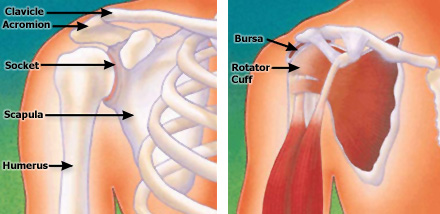
Anatomy
The shoulder joint has three bones: the shoulder blade (scapula), the collarbone (clavicle), and the upper arm bone (humerus). The head of the upper arm bone (humeral head) rests in a shallow socket in the shoulder blade called the glenoid. The head of the upper arm bone is usually much larger than the socket, and a soft fibrous tissue rim called the labrum surrounds the socket to help stabilize the joint. The rim deepens the socket by up to 50% so that the head of the upper arm bone fits better. In addition, it serves as an attachment site for several ligaments.
Risk Factors/Prevention
Injuries to the tissue rim surrounding the shoulder socket can occur from acute trauma or repetitive shoulder motion. Examples of traumatic injury include:
• Falling on an outstretched arm
• A direct blow to the shoulder
• A sudden pull, such as when trying to lift a heavy object
• A violent overhead reach, such as when trying to stop a fall or slide
• Throwing athletes or weightlifters can experience glenoid labrum tears as a result of repetitive shoulder motion.
Symptoms
The symptoms of a tear in the shoulder socket rim are very similar to those of other shoulder injuries. Symptoms include
• Pain, usually with overhead activities
• Catching, locking, popping, or grinding
• Occasional night pain or pain with daily activities
• A sense of instability in the shoulder
• Decreased range of motion
• Loss of strength
Diagnosis
If you are experiencing shoulder pain, your doctor will take a history of your injury. You may be able to remember a specific incident or you may note that the pain gradually increased. The doctor will do several physical tests to check range of motion, stability, and pain. In addition, the doctor will request x-rays to see if there are any other reasons for your problems.
Because the rim of the shoulder socket is soft tissue, x-rays will not show damage to it. The doctor may order a computed tomography (CT) scan or magnetic resonance imaging (MRI) scan. In both instances, a contrast medium may be injected to help detect tears. Ultimately, however, the diagnosis will be made with arthroscopic surgery.
Tears can be located either above (superior) or below (inferior) the middle of the glenoid socket.
A SLAP lesion (superior labrum, anterior [front] to posterior [back]) is a tear of the rim above the middle of the socket that may also involve the biceps tendon.
A tear of the rim below the middle of the glenoid socket that also involves the inferior glenohumeral ligament is called a Bankart lesion.
Tears of the glenoid rim often occur with other shoulder injuries, such as a dislocated shoulder (full or partial dislocation).
Treatment
Until the final diagnosis is made, your physician may prescribe anti-inflammatory medication and rest to relieve symptoms. Rehabilitation exercises to strengthen the rotator cuff muscles may also be recommended. If these conservative measures are insufficient, your physician may recommend arthroscopic surgery.
During arthroscopic surgery, the doctor will examine the rim and the biceps tendon. If the injury is confined to the rim itself, without involving the tendon, the shoulder is still stable. The surgeon will remove the torn flap and correct any other associated problems. If the tear extends into the biceps tendon or if the tendon is detached, the shoulder is unstable. The surgeon will need to repair and reattach the tendon using absorbable tacks, wires, or sutures.
Tears below the middle of the socket are also associated with shoulder instability. The surgeon will reattach the ligament and tighten the shoulder socket by folding over and "pleating" the tissues.
Rehabilitation
After surgery, you will need to keep your shoulder in a sling for 3 to 4 weeks. Your physician will also prescribe gentle, passive, pain-free range-of-motion exercises. When the sling is removed, you will need to do motion and flexibility exercises and gradually start to strengthen your biceps. Athletes can usually begin doing sport-specific exercises 6 weeks after surgery, although it will be 3 to 4 months before the shoulder is fully healed.
Rotator Cuff Tears
• Anatomy
• Cause
• Symptoms
• Diagnosis
• Nonsurgical Options
• Surgical Treatment
• Rehabilitation
• Research on the Horizon
The rotator cuff is the network of four muscles and several tendons that form a covering around the top of the upper arm bone (humerus). These muscles form a cover around the head of the humerus. The rotator cuff holds the humerus in place in the shoulder joint and enables the arm to rotate.
Rotator cuff tear is a common cause of pain and disability among adults. Most tears occur in the supraspinatus muscle, but other parts of the cuff may be involved.
Anatomy
| The rotator cuff helps to lift and rotate the arm and to stabilize the ball of the shoulder within the joint. The rotator cuff is made up of four muscles and their tendons. These combine to form a " cuff " over the upper end of the arm (head of the humerus).
The four muscles of the cuff (supraspinatus, infraspinatus, subscapularis, and teres minor muscles) are attached to the scapula on the back through a single tendon unit. The unit is attached on the side and front of the shoulder on the greater tuberosity of the humerus. |
|
| |
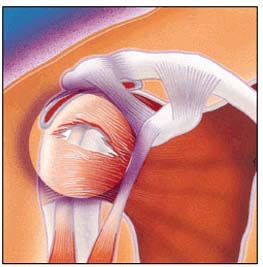
The rotator cuff covers the head of the humerus and stabilizes the shoulder joint.
|
Cause
| The rotator cuff can be torn from a single traumatic injury. Patients often report recurrent shoulder pain for several months and a specific injury that triggered the onset of the pain. A cuff tear may also happen at the same time as another injury to the shoulder, such as a fracture or dislocation.
Most tears, however, are the result of overuse of these muscles and tendons over a period of years. People who are especially at risk for overuse are those who engage in repetitive overhead motions. These include participants in sports such as baseball, tennis, weight lifting, and rowing.
Rotator cuff tears are most common in people who are over the age of 40. Younger people tend to have rotator cuff tears following acute trauma or repetitive overhead work or sports activity.
Rotator cuff tear may often happen as a result of wear and tear.
|
|
| |
A tear can occur within the muscle. |
Symptoms
Some of the signs of a rotator cuff tear include:
Atrophy or thinning of the muscles about the shoulder
Pain when lifting the arm
Pain when lowering the arm from a fully raised position
Weakness when lifting or rotating the arm
Crepitus or crackling sensation when moving the shoulder in certain positions
Symptoms of a rotator cuff tear may develop right away after a trauma, such as a lifting injury or a fall on the affected arm. When the tear occurs with an injury, there may be sudden acute pain, a snapping sensation and an immediate weakness of the arm. Symptoms may also develop gradually with repetitive overhead activity or following long-term wear. Pain in the front of the shoulder radiates down the side of the arm. At first, the pain may be mild and only present with overhead activities, such as reaching or lifting. It may be relieved by over-the-counter medication such as aspirin or ibuprofen.
Over time the pain may become noticeable at rest or with no activity at all. There may be pain when lying on the affected side and at night.
Diagnosis
Diagnosis of a rotator cuff tear is based on the symptoms and physical examination. X-rays, and imaging studies, such as MRI (magnetic resonance imaging) or ultrasound, are also helpful.
Your doctor will examine the shoulder to see whether it is tender in any area or whether there is a deformity. He or she will measure the range of motion of the shoulder in several different directions and will test the strength of the arm. The doctor will also check for instability or other problems with the shoulder joint.
| The doctor may also examine the neck to make sure that the pain is not coming from a " pinched nerve " in the cervical spine and to rule out other conditions, such as osteoarthritis or rheumatoid arthritis.
Plain X-rays of a shoulder with a rotator cuff tear are usually normal or show a small spur. For this reason, the doctor may order an additional study, such as an ultrasound or MRI. These can better visualize soft tissue structures such as the rotator cuff tendon.
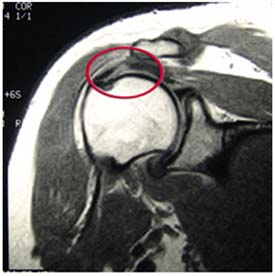
An MRI can sometimes tell how large the tear is, as well as its location within the tendon itself or where the tendon attaches to bone.
|
|
| |
Magnetic resonance image shows a
full-thickness rotator cuff tear within the tendon. |
Nonsurgical Options
In many instances, nonsurgical treatment can provide pain relief and can improve the function of the shoulder.
Nonsurgical treatment options may include:
• Rest and limited overhead activity
• Use of a sling
• Anti-inflammatory medication
• Steroid injection
• Strengthening exercise and physical therapy
Surgical Treatment
Your orthopaedic surgeon may recommend surgery if
• Nonsurgical treatment does not relieve symptoms
• The tear has just occurred and is very painful
• The tear is in the shoulder of the dominant arm of an active person
• If maximum strength in the arm is needed for overhead work or sports
The type of surgery performed depends on the size, shape, and location of the tear. A partial tear may require only a trimming or smoothing procedure, called a " debridement. " A complete tear within the thickest part of the tendon is repaired by suturing the two sides of the tendon back together. If the tendon is torn away from where it inserts into the bone of the arm (humerus), it is repaired directly to bone.
Many surgical repairs can be done on an outpatient basis.
In the operating room, your surgeon may remove part of the front portion of the scapula, the acromion as part of the procedure. The acromion is thought to cause " impingement " on the tendon. This may lead to a tear. Other conditions such as arthritis of the AC joint or tearing of the biceps tendon may also be addressed.
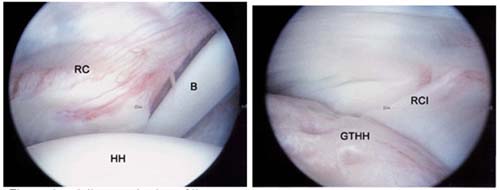
|
Left, Arthroscopic view of the rotator cuff from within the joint shows the rotator cuff (RC),
the head of the humerus (HH), and the biceps tendon (B). |
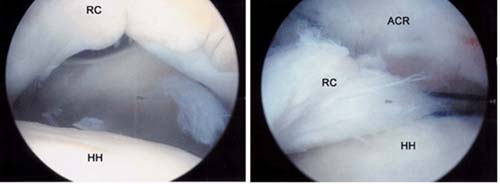
|
Left, Arthroscopic view of rotator cuff tear. A large gap can be seen between the
edge of the rotator cuff and humeral head. |
In general, three approaches are available for surgical repair. These include:
• Arthroscopic Repair. A fiberoptic scope and small, pencil-sized instruments are inserted through small incisions instead of a large incision. The arthroscope is connected to a television monitor and the surgeon can perform the repair under video control.
• Mini-Open Repair. Newer techniques and instruments allow surgeons to perform a complete rotator cuff repair through a small incision, typically 4 cm to 6 cm.
• Open Surgical Repair. A traditional open surgical incision is often required if the tear is large or complex or if additional reconstruction, such as a tendon transfer, has to be done. In some severe cases, where arthritis has developed, one option is to replace the shoulder joint.
Top of page
Rehabilitation
After surgery, the arm is immobilized to allow the tear to heal. The length of immobilization depends upon the severity of the tear. An exercise program will help regain motion and strength in the shoulder. This program begins with passive motion and advances to active and resistive exercises. Complete recovery may take several months.
• A strong commitment to rehabilitation is important to achieve a good surgical outcome. The doctor will examine the outcome to advise when it is safe to return to overhead work and sports activity.
|